Chronic pancreatitis in the paediatric demographic presents a formidable clinical challenge. Characterized by debilitating abdominal pain, progressive glandular fibrogenesis, and subsequent exocrine and endocrine insufficiency, the condition severely impacts a child’s quality of life and developmental trajectory. For effective pain relief and ductal decompression, the Frey procedure – comprising a local resection of the pancreatic head combined with a longitudinal pancreaticojejunostomy – remains a gold-standard surgical intervention.
However, transitioning this complex reconstruction to a minimally invasive robotic platform requires an exceptional degree of surgical expertise and technological integration.
Inherent Complexities Of The Frey Procedure
The Frey procedure is inherently demanding due to the intricate and highly vascularized anatomy of the hepatobiliary and pancreatic systems.
The primary clinical objective is to radically core out the diseased, calcified tissue of the pancreatic head while meticulously preserving the duodenum, the biliary tree, and the posterior pancreatic capsule. Navigating this surgical plane requires acute awareness of local vasculature and biliary structures, making the margin for error virtually non-existent.
Anatomical Hurdles In Paediatric Patients
Adapting this intervention for a paediatric cohort amplifies the surgical difficulty exponentially. Executing this surgery robotically in a child is extraordinarily demanding primarily due to the inherent fragility of the juvenile pancreatic anatomy. Surgeons are forced to navigate an exceedingly confined operative workspace. Furthermore, the procedure mandates meticulous, watertight reconstruction in immediate proximity to critical vascular networks and delicate ducts.
Paramount to the procedure’s long-term success is the absolute precision required to excise the fibrotic tissue while maximally preserving the surrounding viable pancreatic parenchyma, thereby safeguarding the child’s future metabolic and digestive functions.
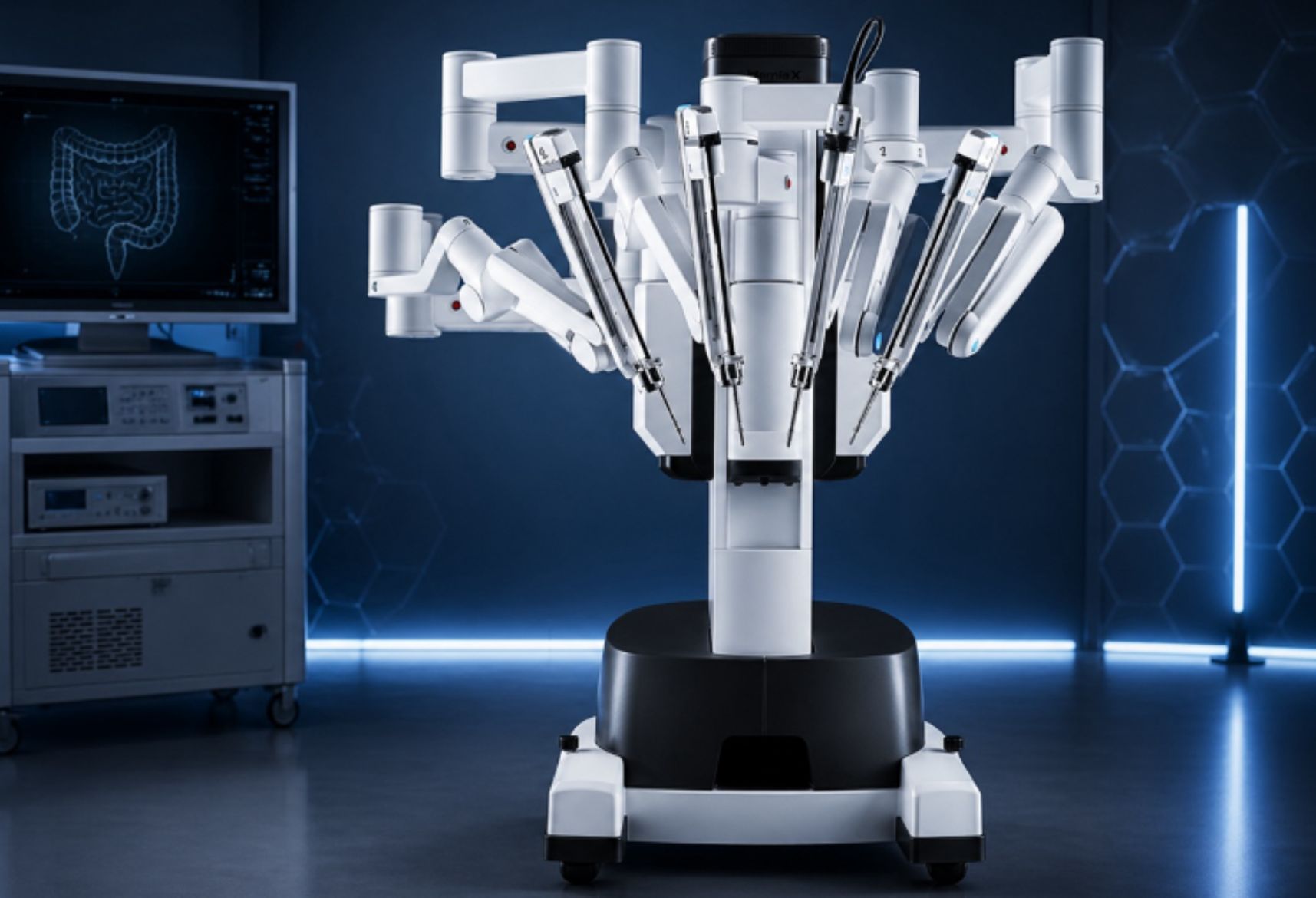
The Da Vinci Advantage In Reconstructive Surgery
To overcome the severe anatomical constraints of paediatric patients, the integration of cutting-edge surgical technology is not just beneficial, but essential. Utilizing platforms like the Da Vinci Robotic Surgical System fundamentally transforms the operative approach. This sophisticated robotic equipment equips operating surgeons with unparalleled biomechanical advantages during the high-stakes reconstructive phases of the surgery.
It delivers a high-definition, magnified 3D spatial visualization of the operative field, providing the vital depth perception necessary for safe micro-dissection around the portal vein and mesenteric vessels.
Additionally, the system’s advanced algorithmic software provides seamless tremor filtration, translating the surgeon’s macroscopic hand movements into highly precise micro-movements at the tissue level.
The articulated, wristed instruments grant superior dexterity and degrees of freedom that far surpass traditional laparoscopy.
This enhanced articulation is particularly crucial when executing the complex, multi-layered suturing required for a secure pancreaticojejunal anastomosis within a restricted paediatric abdominal cavity.
Securing Superior Clinical Outcomes
In conclusion, the robotic-assisted Frey procedure represents a significant milestone in the surgical management of paediatric chronic pancreatitis.
By synergizing elite surgical proficiency with the biomechanical superiority and precision of advanced robotic systems, multidisciplinary healthcare teams can effectively navigate the unique anatomical hurdles of children.
This technological synergy minimizes operative trauma, accelerates postoperative recovery, and ultimately secures superior long-term clinical outcomes for a highly vulnerable patient population.
Authored by:
Dr Senthil Gnanasekaran
Clinical Lead, Abdominal Organ Transplant & HPB Surgery (Liver, Kidney, Pancreas & Small Intestine)
Dr Senthil Gnanasekaran is a renowned hepatopancreatobiliary and liver transplant surgeon with distinguished expertise in both living and deceased donor liver transplantation. His proficiency extends to advanced procedures for complex liver, pancreatic, and biliary disorders, combining the latest minimally invasive, laparoscopic, and robotic techniques to ensure the best possible outcomes.
As a clinical leader, Dr Senthil is deeply committed to comprehensive transplant care, prioritising patient safety using world-class surgical care and multidisciplinary collaboration throughout the treatment journey. He is especially skilled in managing advanced liver disease and complex gastrointestinal conditions, providing tailored solutions with a focus on quality of life.
Dr. Piyush Bawane
Clinical Lead, Medical Gastroenterology.
Dr Piyush Bawane is a highly motivated and compassionate gastroenterologist with over a decade of experience in medical gastroenterology and interventional endoscopy, including ERCP and EUS.
He is skilled in advanced procedures and gastric motility studies, with a strong focus on the management of gastrointestinal and liver diseases.
He is proficient in the evidence-based management of gastrointestinal and liver diseases and has extensive experience in handling complex and challenging GI disorders.
Alongside his clinical practice, Dr Bawane is actively involved in several arcademic associations and professional organizations. He has contributed to multiple research studies in gastroenterology and has published widely in national and international journals.